A 54-year-old chronic smoker presented with a sudden onset of left-sided chest pain, which was heaving in nature. He was fully conscious with stable vital signs. His physical examination was unremarkable. His first electrocardiogram (ECG) showed upsloping ST segment depression in V4–V5, symmetrical tall T-wave in V4 and ST segment elevation in aVR. These ECG findings were consistent with de Winter pattern. His ECG also showed prominent T-waves in V2–V3 and ST depression in II, III and aVF. Subsequently, a repeat ECG upon arrival at the hospital did not exhibit similar findings. His troponin I was markedly raised, which was more than 10 ng/ml (normal < 0.02 ng/ml).
Figure 1 First ECG
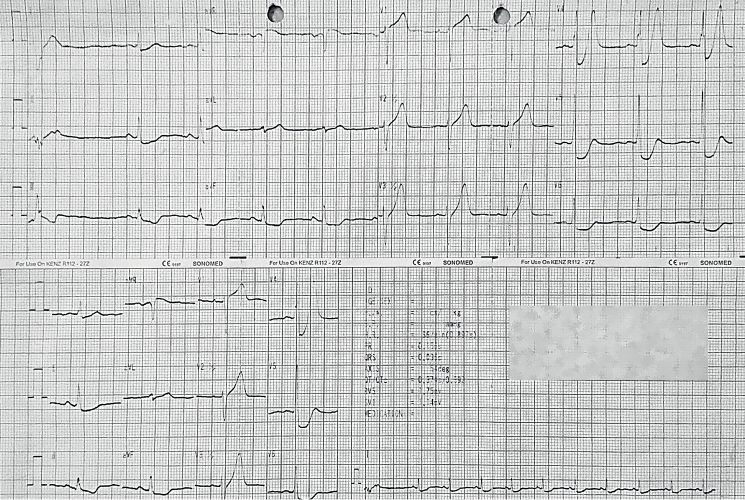
Figure 2 Evolution of ECG before and after PCI
His echocardiogram revealed a left ventricle ejection fraction (LVEF) of 30% with almost global hypokinesia. The angiogram showed a severe three-vessel disease with left main coronary artery (LMCA) lesion. The LMCA to left anterior descending artery (LAD) and right coronary artery (RCA) were stented with everolimus-eluting stents. He remained angina free and was discharged well two days after the percutaneous coronary intervention.
ST elevation myocardial infarction (STEMI) ECGs are well recognised. However, ’STEMI-equivalent’ ECG patterns without typical ST segment elevation may pose a daunting task for prompt diagnosis. Several STEMI-equivalent ECG patterns have been described:1
- de Winter pattern
- ST elevation in aVR
- Pathological ST elevation in the presence of left bundle branch block
- Wellens’ phenomenon.
de Winter ECG pattern was first described by de Winter et al. in 2008, which accounts for 1.6%–2.0% of acute occlusion of the LAD resulting in anterior myocardial infarction.2,3 Up to 27% of mortality within the first week was reported in this ECG pattern.3 de Winter et al. recorded this ECG pattern on average 1.5 hours after the onset of the symptom.2 The first ECG of our case, which was recorded at four hours after the onset, exhibited the typical de Winter ECG pattern. However, another ECG done in the hospital (5.5 hours after the onset) evolved. Therefore, it is crucial for clinicians not to dismiss any previous ECGs, and to compare and follow up with serial ECGs.
Prominent T-wave and ST-segment depression, instead of classical ST-segment elevation in critical stenosis of the LAD, is postulated to occur due to delay in repolarisation in the subendocardial region, with a change in the transmembrane action potential shape.4 This ECG pattern is typically associated with LAD involvement without an LMCA lesion.2 Our case, however, demonstrated a significant LMCA and LAD disease. This is in line with another case report of de Winter ECG pattern in a patient with a total occlusion of the LMCA.5
Despite its rarity in day-to-day practice, physicians should be familiar with this type of ECG pattern and have a high index of suspicion to prevent any treatment delay. 
References
- Lawner BJ, Nable JV, Mattu A. Novel patterns of ischemia and STEMI equivalents. Cardiol Clin 2012; 30: 591–9.
- de Winter RJ, Verouden NJW, Wellens HJJ, Wilde AAM. A new ECG sign of proximal LAD occlusion. N Engl J Med 2008; 359: 2071–3.
- de Winter RW, Adams R, Amoroso G et al. Prevalence of junctional ST-depression with tall symmetrical T-waves in a pre-hospital field triage system for STEMI patients. J Electrocardiol 2019; 52: 1–5.
- Fiol Sala M, Bayes de Luna A, Carrillo Lopez A et al. The ‘de Winter pattern’ can progress to ST-segment elevation acute coronary syndrome. Rev Esp Cardiol (Engl Ed) 2015; 68: 1042–3.
- Zhan ZQ, Li Y, Wu LH, Han LH. A de Winter electrocardiographic pattern caused by left main coronary artery occlusion: a case report. J Int Med Res 2020; 48: 300060520927209.