



Support us
As a charity we rely on your donations to fund our free exhibitions, school activities and online resources
To cite this article: Malcolm Nicolson, 'Ian Donald, Diagnostician and Moralist', online publication, Royal College of Physicians of Edinburgh (2000)

The population of Scotland is divided into two halves. We are irrevocably separated by a dichotomy that transcends mere petty issues of creed or class and is even largely independent of sporting allegiances. I refer, of course, to that quite irresolvable controversy between those who prefer Glasgow to Edinburgh and those whose loyalties lie in the opposite direction. Since I am here addressing the Glasgow College, I had better make it immediately clear where the preference of my subject, Ian Donald, Regius Professor of Midwifery, lay. Here is his account of a speaking engagement to one of those institutions at the other end of the M8, namely the Scottish Branch of the Royal College of Midwives:
'I began my lecture in a fury at not even having been invited to lunch just before it, the sort of inhospitality for which Edinburgh is famous. I retaliated by eating a picnic lunch in their car park and not walking through the doors of the College until exactly two minutes before I was due to start, by which time the old hags were in a proper tiz about whether I was even going to show up. I will also bill them for 5 hours subsistence ‘in view of the absence of an invitation to lunch’. This sort of meanness could not happen in Glasgow or Dublin.'
The letter was to an Irish correspondent, which explains the reference to Dublin.
This quotation, I think, displays many of Donald’s qualities - in particular his idiosyncratic mixture of personal courtesy and very considerable forthrightness of expression. Not to mention - how shall I put it? - what we might call a certain old-fashioned sexism.
The passage immediately before this one in the same letter is also illuminating as to his character:
'As you gather I am out of hospital and trying to get going again. Yesterday I made my first public effort with an hour’s lecture in Edinburgh to an audience of 100 midwives at the R.C.M. and timed it exactly to the minute and found myself on my old form although feeling very breathless and suffering considerably from my back.'
Donald was in fact recovering from what was merely the latest episode of a life-long struggle with valvular disease of the heart. He was also, at the time of his Edinburgh trip, suffering from a slipped disc. Sixty-eight years old, Donald had, in the preceding four years, undergone the third of his major heart operations, to remove a mitral homograft and replace it with a Starr Edwards artificial valve; hospitalisation and a full dental clearance (which required a stay in the intensive care unit because of his anticoagulant regime) for recurrent sub-acute bacterial endocarditis; and the excision of a squamous cell carcinoma from his right hand. He would soon have to submit to surgical repair of a rapidly enlarging inguinal hernia (a common sequel of cardiopulmonary bypass in those days). In August 1978, he was not, by any criterion, a well man. These passages thus also speak of Donald’s great physical courage and his immense determination.
Donald’s courage is also evident, I think, in the following passage, written in his retirement capacity as a consultant for the ultrasound manufacturer, Nuclear Enterprises:
'[T]he ‘spinner’ [a real-time ultrasound machine] was got going very well and here my own heart with its signs of incipient cardiac failure with distended inferior vena cava measuring impressively at 2.65 cms, and later even more, and my engorged hepatic veins showed up beautifully and impressed (and depressed) even me. My deformed tricuspid valve and mitral prosthesis came up well as did also my right kidney and I soon got very practised at slick demonstration including my pancreas and superior mesenteric artery and I encouraged bystanders to have a ‘go’ at examining me.'
This quotation also evinces, I would argue, Donald’s fascination, even into his retirement, with the technology of diagnosis and indeed with the activity of diagnosis itself – the great intellectual and practical adventure of conceptualising what is going on inside the human body.
Of course, as I make these judgements about Donald’s character and his interests, I am aware that there are those in the audience who knew Ian Donald personally and who could thus speak about aspects of his personality with greater authority than I can claim. But what I hope to offer tonight, if it does not sound too pretentious, is what one might call a historian’s first draft – in essence I wish to indicate how the historian assembles his account of his subject by the assessment and interpretation of the available evidence – by the study of archival sources such as I have already quoted from, and, of course, from listening to the testimony of those who did have personal experience of the subject.
This is a section of a transcript from an interview with Ian Donald’s sister, Dame Alison Munro:
'Yes, he [Ian Donald] had a very great friend, Dennis Hill who became Sir Dennis Hill, President of the Royal College of Psychiatrists, at St Thomas's … and he and Dennis were great friends and it was after the war when people didn't know what was going to happen and he did consider it [becoming a psychiatrist]. I think becoming a gynaecologist was a second choice for him.'
Which makes an interesting observation.
Despite my title, I am not really going to say much in detail about Donald’s diagnostic practice. That, I fear, would be presumptuous of me in front of the present audience. But what I am however going to do is to argue that there was a connection between Donald’s attitude to diagnosis and his general moral outlook. Not a necessary or logical link, of course, but a real historical connection nevertheless.
Here is a brief outline of Donald’s career:
Born in Cornwall in 1910
Brought up in South Africa, attended the University of Capetown, studied Music, Classics and French, graduated with First Class Honours in Arts
Studied medicine at St Thomas’s in London – graduated 1937
While a medical student, invented a machine for rinsing out the urinary bladder War service as a Medical Officer in the RAF
1946-54 - Registrar at St Thomas’s and Reader at the Royal Postgraduate Medical School, Hammersmith - Invented a mechanical respirator for neonates
1954-1976 – Regius Professor of Midwifery at the University of Glasgow
In this last capacity, Donald led the team of clinicians and engineers who established ultrasound as a clinically useful imaging modality in gynaecology and obstetrics. Their first major publication appeared in 1958 and contained the first ultrasound images of the fetus ever published. In the 1970’s, Donald worked on the development of the Ovutector, an electronic aid to ‘natural’ contraception.
Now there is an understandable tendency, not so much in Glasgow perhaps, but certainly in the wider literature on ultrasound for Donald to be presented purely as a technological innovator. But, as his former colleagues will know well, that is by no means a full description of Donald. As we have noted already, Donald had a broad education in Arts; indeed he must have been one of very few medical students of his generation with a thorough grounding in the Classics. To the end of his life, he enjoyed displaying his Classical learning. Here is the heading of a book review he published in the B.M.J. in 1979:
Ultrasound in Gynecology and Obstetrics. Sam N Hassani (in collaboration with R L Bard.) (Pp 182; $24.80.) Springer. 1978. Practical Abdominal Ultrasound. Constantine Metreweli. (Pp 121; 17 plates; £12.50.) William Heinemann Medical Books. 1978.
A User’s Guide to Diagnostic Ultrasound. Isabel M Shirley, Roland J Blackwell, Geoffrey Cusick, David J Farman, and F Robin Vicary. (Pp 329; £12.) Pitman Medical. 1978.
Arbiter es fonnae, certamina siste dearum.
Vincere quae forma digna sit una duas.
OVID
(Thou art the judge of beauty; quell thou the
strifes of the goddesses.
Which one in beauty deserves to score over the
other two?)
You can see the quotation from Ovid – helpfully translated into English below for those of us without the benefit of a Classical education.
Donald liked to display his knowledge not merely of Classical literature but of English and French literature as well. He spoke and wrote French quite fluently. He read Italian. He wrote to his Norwegian grandchild in Norwegian. He was an accomplished watercolourist and a skilled pianist. After his heart operations he gauged his return to health using a quite precise means of clinical assessment but one that, I suspect, he did not impose upon many of his own patients:
'I can play the last movement of Beethoven’s Moonlight Sonata at near regulation speed without having to stop because of breathlessness – a good yardstick.'
In this sense Donald is a link to the time, not so very long ago, when elite physicians prided themselves on their possession of ornamental culture as well as professional learning. One might here think of the leaders of the profession in the inter-war period, men such as Lord Horder of Barts Hospital, for example. Tommy Horder will, I think, be known by reputation to most of the medical members of my audience and it will be recalled that he did not retire until 1936 and lived until 1955.
I mention Horder deliberately because he and his elite colleagues in the London teaching hospitals in the Edwardian and inter-war periods have recently been the subject of an intriguing series of studies by the historian of medicine, Christopher Lawrence. Professor Lawrence identifies Horder as what he calls a ‘clinical holist’. Here are some of the defining characteristics of clinical holists, as described by Lawrence.
Clinical Holists, e.g. Lord Horder,
Displayed wide learning and culture outside of medicine
Valued breadth of experience in medicine
Celebrated bedside diagnostic skill as central to medicine
Gave only conditional approval of laboratory-generated knowledge
Disdained abstractions
Took a cautious attitude to instrumentation and technology
Disdained organ-specific specialisation
Regarded disease as disturbance of whole body – holistic clinical focus
Espoused hierarchical professional and social attitudes
Presented the clinician as a defender of moral value
I broadly agree with the thrust of Professor Lawrence’s argument that this constellation of views functioned as a professional credo, what one might call an ideology, for the leading clinicians of the London teaching hospitals, the ‘Greats’ as they were called, in the first half of the twentieth century.
Ian Donald, it will be recalled, was a student at St Thomas’s at the time when the influence of Horder and his like was still being felt. Of course in many respects the differences between Donald and Lord Horder are enormous – Horder had one of the most lucrative and socially exclusive private practices in London; Donald was proud of the fact that he worked for the NHS and could and would treat, as he put it, ‘every mother like a Duchess’. Donald embodied an ethos of professional salaried public service that would have been quite alien to Horder and his ilk, who measured their professional worth by their private practices and the prestigious posts they occupied, unpaid, in the voluntary hospitals. And yet, there are intriguing similarities between the two men, which are worth exploring if a full characterisation of Donald as a medical thinker is to be achieved. It is particularly worth noting what Lawrence says about clinical holists as defenders of moral value. And we have already noted the importance Donald placed on a broad education outside of medicine.
What Lawrence argues is, in essence, that there is quite a specific historical connection between Horder’s views on social and cultural matters, on the one hand, and his medical practice as an elite clinician, on the other. What I wish to argue here, indeed what the title of my lecture is intended to imply, is that a similar, if by no means identical, thesis can be advanced with regard to Donald.
In this respect, one can, of course, learn a lot about a person by noting the company they keep:

This photograph was taken at the opening of the new maternity hospital, The Queen Mother’s Hospital, in 1964. Donald was responsible for much of its design, down to the situation of the wards and the detailed layout of the labour rooms. He personally recruited many of the staff. It was very much his ‘baby’, as one of his obituarists put it. He insisted that the new hospital be named after the Queen Mother, whom he greatly admired, and that she be invited to open it. Years later, at a reception in the Royal College of Obstetricians and Gynaecologists, he was equally delighted to be recognised by, kissed by, and photographed with, the Princess of Wales.
Here is a picture of Donald with the Duke and Duchess of Kent.

He was a personal friend of the Kents and acted as something of a personal advisor to the Duchess. She and he shared opinions on a number of matters.
Donald was, it is fair to say, a royalist. In later years he yearned for the knighthood he was fated never to receive. Donald was also an active member of the Scottish Episcopal Church – the Anglican Church in Scotland. He was fairly High Church and while, as far as I am aware, he never actually described himself as Anglo-Catholic, that was broadly his doctrinal position.

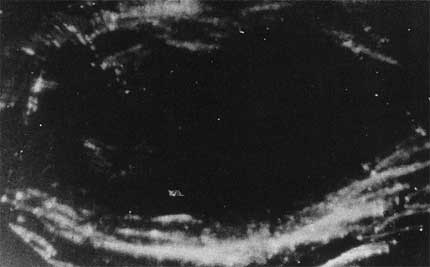
Let us now move on to consider some examples of Donald’s medical discourse. Here is an excerpt from a lecture on obstetric ultrasound that Ian Donald gave to a medical audience in 1978:
'…You can see quite easily here, the head of the baby above…the eye sockets, the nose, cheeks, chin, the neck, the thorax of the baby, the heart, and the rest of it floats away into a third dimension. It is also sitting on top of its own placenta, which is quite common at this stage of pregnancy … She is a woman with a very bad obstetric history, and the baby is now a beautiful child of three. I had to deliver her by caesarean section – charming child, but not so beautiful as here'.
I believe that this is the image that was being shown by Donald on that occasion.

One could point to several features of this quotation which are instructive about the character of Donald’s involvement with the imaging technology he had been very largely responsible for developing. First of all, and obviously, the ultrasound scan allows the visualisation of the fetus in detail in utero. But more than that – not merely the visualisation but what one might call the individualisation – it allows the fetus to be recognised as, or at least spoken of as, an individual. In Donald’s account, the child of three and the fetus both have recognisably personal characteristics – one is charming, the other more beautiful still.
One might also note the way Donald moves from discussion of the fetus to discussion of the mother and back again. One might be forgiven for a brief moment of confusion as to whom the ‘she’ in the fifth line refers. Mother and baby are muddled up, as it were – Donald’s account moves from one to the other without signposting the shift. One gets a strong sense that mother and fetus are, in Donald’s mind at least, the one clinical unit and yet at the same time, as we have noted, the fetus is itself also a distinct individual in its own right.
When called upon to reflect upon his choice of career in obstetrics, Donald used to say, as we have already noted, that the only other specialty he had ever seriously contemplated was psychiatry. What do obstetrics and psychiatry have in common? In Donald’s view, they both dealt with whole patients, with complete individuals, rather than with the isolated bits of the body that were, as he saw it, the professional domain of, say, the cardiologist or the hepatologist. And, as Donald presented it, the advantage of obstetrics over psychiatry was that, in his particular line of medical business, the clinician had not one whole patient but two whole patients, mother and fetus both. In this sense at least Donald was certainly a clinical holist.
What is also evident I think from this quotation is the enthusiasm with which Donald displays the image of the intrauterine fetus. To Donald, pointing to the details of the developing individual in this way was a matter of great pride, a triumphant culmination of his life’s work in obstetrics.
Donald took pride in the fact that he had launched, as he put it, a ‘new diagnostic science’, with the emphasis very strongly on the word diagnostic. This stress on diagnosis is particularly telling in that it distinguishes Donald from some of the other pioneers of ultrasound imaging, notably Douglas Howry in America. Howry was mostly interested in using ultrasound to reveal underlying structure. Effectively he sought to use the modality to provide what one might call a better x-ray.

These pictures, marvellous technical achievements as they were, had little or no clinical relevance. But, even as a technological innovator, Donald was, first and foremost, a clinician among clinicians – he sought, as I say, not to provide better pictures but better diagnoses.
The other major American-based pioneer of ultrasonography to rank beside Douglas Howry was John Wild. Again Donald contrasted his style of investigation with Wild’s:
'Wild, for example, sought to measure the thickness of bowel wall and hence signs of carcinomatous ulceration of the stomach using a quartz transducer within the lumen of the gut. His experiments were carried out on dead dogs’ intestines and post-mortem material. Having never had to waste time myself on animals and corpses, both of which I detest in experimental work, I was able to cut a lot of corners which they had first to round … As soon as we got rid of the backroom attitude and brought our apparatus fully into the department with an inexhaustible supply of living patients with fascinating clinical problems we were able to get ahead really fast.'
Effectively Donald’s argument was that Wild was dealing with laboratory abstractions, whereas he (Donald) was engaged with the concrete problems presented by the clinical situation. Actually I am not sure that Donald is here being wholly fair to Wild but again it is an example of how Donald presented himself not as merely a technological innovator but rather as a clinical innovator, as a diagnostician among diagnosticians.
Donald was very proud of the diagnostic distinctions that his new apparatus allowed him to make. It is worth emphasising that, initially at least, the images obtained with obstetric ultrasound were often very difficult to interpret. Very considerable diagnostic skill was required to ascertain their full clinical significance.
This, for example, is a very early image of a fetus at just nine weeks gestation. This fetus was found more or less by accident in the womb of a woman who had three months of irregular vaginal bleeding and a hard enlargement of the uterus. The patient had a previous history of fibroids and was admitted to the Western Infirmary for the surgical removal of a suspected myoma. She was examined by Ian Donald with his new-fangled scanner and the image you can see here was obtained. You can see that the uterus is enlarged with fluid and here in the left hand corner can be discerned the faint echoes of what Donald was convinced was a fetus, or at least a gestational sac, despite the fact that the woman had no breast symptoms and did not think she could be pregnant. A pregnancy test was ordered. The results were eagerly awaited and sure enough Donald’s opinion was confirmed. Bed rest cured the bleeding and in due course she was delivered of a healthy baby. This case was a real diagnostic coup for Donald and for ultrasound since the best diagnosis that could be arrived at by conventional clinical means was undoubtedly myoma.
Donald and his team scored many impressive diagnostic coups over their clinical colleagues with their ability to produce and correctly to interpret these sort of images. Indeed the subtext on several of Donald’s early publications can be read as points scoring against his sceptical colleagues in diagnostic controversies. As this extract from one of his articles in the American Journal of Obstetrics and Gynaecology illustrates:
'Patient 2 days post partum with a large, flaccid abdomen clinically diagnosed as due to ascites. Top left picture shows transverse section of a large clear cyst … Ultrasonic diagnosis was discounted and the patient dismissed to attend an Outpatient Clinic. She was admitted to another hospital a few days later with acute abdomen due to massive infarction of the cyst.'
These episodes were important to Donald because a number of his fellow obstetricians expressed scepticism about the clinical value of ultrasound. Over in that infamously inhospitable medical centre in Mid-Lothian, a professor of obstetrics used to amuse local audiences by announcing that, in Glasgow, they had invented a £10,000 machine to undertake a task that, in Edinburgh, was routinely accomplished with the aid of a tuppenny rubber glove. In this case, as Donald is clearly pleased to point out, the machine certainly vanquished the glove.
In Donald’s view, however, the production of ultrasound images could not make diagnosis so simple as to reduce it to merely a technical exercise. On the contrary, Donald argued, the images still needed a skilled interpreter. Indeed, in Donald’s usage, ultrasound technology enhanced rather than diminished the role for the craft skill of the diagnostician. In other words, the new machines enhanced rather than diminished the ability of the clinician to cultivate and display diagnostic acumen at the bedside. As he put it, and note the literary allusion:
'Ay! There’s the rub. A new diagnostic dimension has been added, but the days of push-button diagnosis are no nearer. The case for sonar may be dangerously overstated and clinical observation and common sense are still paramount'.
Incidentally Donald, virtually to the end of his days, persisted in calling ultrasound ‘sonar’.
Donald encouraged radiologists to take an interest in ultrasound in order to develop its potential in other areas of medicine. The remarkable achievements of his colleague, the radiologist Patricia Morley, gave him considerable satisfaction. But Donald nevertheless sought to keep obstetric applications of the technology firmly under the control of obstetricians, as the following quotation illustrates:
'… sonar, like radiology and biochemistry, must never lose their [sic] subservience to the medical art and the paramount importance of the patient who is the clinician’s chief concern. Viewed in this sense of proportion, sonar comes as a commodity only, though one with many uses. Out of control it can become an obsession, a tail that wags the whole dog … Sonar is not a new medical religion like acupuncture or homeopathy, nor an end in itself. A tool exploited for its own sake is no better than a saw given to a small boy for cutting wood who must presently look around the house for suitable objects of furniture inviting amputation.'
And again
'Research is always best done directly with the patient, where possible by the patient, or at least with active co-operation and always, repeat always, for the benefit of the patient. This is where technology ends and medicine begins'.
Those of you who know Lawrence’s papers on clinical holism will have seen similar sentiments expressed with regard to medical technology by his subjects. To Horder, for example, it was diagnostic skill at the bedside that was the defining quality of the elite physician: laboratory diagnostic procedures were always secondary to, and subservient to, clinical diagnosis.
It was not, however, only to his clinical colleagues that Donald showed his images of the living fetus. Here is an excerpt from a speech he gave to a lay audience in 1978. He was showing the meeting one of the earliest real-time films of fetal movement:
'Here’s the baby see how he jumps … This baby is about a 12 week pregnancy … she has only missed two periods. She does not even know she is pregnant. She certainly cannot feel these movements but there is no doubt about the reality, … now you see it move its hand up to its face you see his head is up here and his chest is down here then he throws his legs out and his arms … You see his hands come up like that. And you see his face here, the back of his head … This is the fluid sac in which he is contained. The full bladder is this way … It is rather like a child on a trampoline, tremendous strength, energy and vitality.'
Again you can see the conflation of mother and fetus as Donald moves seamlessly from one structure to another, from head to fluid sac to full bladder: and simultaneously the strong sense of the individuality and identity of the fetus, with its ‘strength, energy and vitality’.
Donald draws from this identifiable individuality of the early fetus a strong moral message:
'Anybody who says this is not alive is talking through his neck. It is a lie, which is intolerable and seeing is believing…And one of the things that this film has done if it has done nothing else, is to kill forever the lie of the pro-abortion lobby that there’s nothing there just a potential human being, just – oh look at that jump, he bumps his head against the roof nearly, doesn’t he – This lie that he is just a potential human being when in fact that baby is as human as an old man…the same individual from conception to the grave. And when you destroy a baby by abortion that is what you are destroying. I think you have got to face the fact honestly…There can be no argument about it and if I have done nothing else in my life, I have killed that dirty lie that the foetus is just a nondescript meaningless jelly, disposable at will, something to be got rid of'.
Donald was a committed opponent of the termination of pregnancy for social reasons and he was leading campaigner against the 1967 Abortion Act. In this campaign he employed the ultrasound image as a powerful persuasive resource.
When Donald showed his film to an anti-abortion meeting in Milan in 1979, it caused a very considerable commotion. The Italian debate about abortion reform was in full swing at the time. In the midst of the controversy Donald was invited to an audience with the Pope, a meeting he described as ‘the crowning event of my life’. Donald was particularly impressed that the Pontiff had copies of his ultrasound papers. He was later to describe John Paul II as ‘the greatest man on earth’.
It was not however only to public meetings that Donald showed his images of the living fetus. When he was working in the Queen Mother’s Hospital, Donald would sometimes show ultrasound images to women seeking abortions in a deliberate attempt to deter them from their chosen course of action.
As a colleague described it:
'Then of course you would go and have an ultrasound done and show the mother the picture of this baby you weren’t to murder. This all happened in a busy clinic on a Friday afternoon. So it was full of drama, you were pretty sure of having a couple of dramatic scenes in a Friday afternoon clinic'.
These dramatic scenes were happening, it should be emphasised, before the routine booking-scan was introduced. These were thus scans specially organised solely for the purpose of persuading women to continue with their pregnancies. Donald and his colleagues believed, probably rightly, that many women were indeed deterred from proceeding to abortion as a result of these ultrasound sessions.
The legal situation regarding abortion in Scotland was quite unclear before the 1967 Abortion Act. But even after the 1967 Act clarified the position and put certain categories of abortion upon a firm legal basis, there were very few terminations performed in the departments under Donald’s control. Donald absolutely refused to perform abortions unless the fetus was very grossly deformed. His personal rule was – only ‘when it is cast iron clear that the child is so mentally defective as to be incapable of spiritual development …’ In other words, he was not willing to perform selective abortion in cases of mild or moderate handicap. Indeed Donald’s interventions in pregnancy were all aimed in the opposite direction – toward the preservation of fetal life. He even went to the length of attempting to save an ectopic fetus – a heroic surgical endeavour which ended in failure but which might be taken as symbolic of his attitude regarding the doctor’s proper role with respect to the fetus.
Donald combined strong moral suasion against abortion with a back-up support service for single mothers, which was advanced and comprehensive for the time. Donald was interested in and involved with the social aspects of pregnancy and childcare. This might be seen as another example of his holistic, person-orientated, attitude to clinical practice, which I have already outlined above. When the Queen Mother’s Hospital opened, Donald insisted on the setting up of a medical almoner’s department to provide advice and support to unmarried mothers.
The irony of the story of obstetric ultrasound is, of course, that Donald’s programme to individualise the fetus produced effects quite different to those he had intended. Ultrasound surveillance enhanced, marvellously enhanced, the clinical management of pregnancy. One need only think of the transformation of the management of placenta praevia to be convinced of that. Ultrasonic scanning has also given the fetus a public presence that it could never have had before. Ultrasound images of fetuses have appeared in advertisements and on postage stamps; they regularly illustrate articles in the daily newspapers. The fetus features in a million family albums, pictured apparently as casually as a toddler on the beach.
Seeing images of their fetuses may indeed have deterred many women from having abortions. But as far as the technical context of obstetrics research is concerned, by far the major impact of the ultrasound image has been in intrauterine diagnosis, in the detection of fetal abnormalities. The individualisation of the fetus, the delineation of its individual characteristics, has lead to the ever more detailed scrutiny of fetal structure for pathology. In this area of its use, ultrasound imaging and abortion are not in contention but are indeed complementary. Indeed they are mutually dependent one upon the other. Given that the possibilities of detection far outstrip those of therapy, the only option that can be offered to most of the women who are presented with a diagnosis of fetal abnormality is termination of pregnancy. Research into the detection of fetal abnormality would not have proceeded at anything like the pace it has done, over the last thirty years, if that clinical option had not been readily available. Truly the net effect of the introduction of the ultrasound scanner was the rigorous imposition upon the fetus of a reductionist discrimination between the normal and the pathological, which Donald found morally repugnant. By this we learn, though we knew it before, that the ends to which technology is put cannot be determined by its originators, nor can they be built into machines.
By the 1970’s Donald was aware of this development and was seriously appalled by it. He wrote, ‘My own personal fears are that my researches into early intrauterine life may yet be misused towards its more accurate destruction.’45 And, on another occasion, ‘I myself would not like to feel that I had contributed to a Huxleyian Brave New World.’ He mused as to whether, if he were at the beginning of his medical career rather than at its end, he would again choose obstetrics and gynaecology as a specialty. His dissatisfaction with obstetrics was that the range of concerns of its practitioners had become narrower and more mundane:
'The passage of the Abortion Act in 1967 … is only a signpost in the changing world, a result more than a cause … I think it is necessary for all of us to take close stock of the effect from all that is happening … on ourselves as clinicians who find ourselves willy-nilly at the hub of ethical decisions. The professional status of the gynaecologist is under threat and if we cannot embrace the philosophy and exercise the judgement then we have no right to claim a status much above that of a plumber or a technician.'
Again any one who has read Professor Lawrence’s work on clinical holism will recognise these sentiments – Lord Horder often presented the medical profession as essentially embodying wisdom of a general and reflective rather than a narrowly technical kind. Donald is indeed arguing that these broad concerns ought to be a characteristic of the professional specialty of obstetrics and gynaecology.
Now before I explore these issues further, I must guard against the danger of making Donald sound more of a reactionary then he actually was. Politically he was quite liberal in his views. He voted Tory but not consistently. He and his wife deplored apartheid in South Africa. Nor was Donald elitist or particularly exclusive in all of his social attitudes. He certainly enjoyed the status, power and independence that being a clinical professor in a Scottish university accorded him. But, as I have said, he vigorously supported the National Health Service and took a particular pride in the fact that he never practised privately during his time in Scotland. He was impatient with social pretension and was popular with his working-class Glaswegian obstetric patients. In some respects he could even be, in the eyes of his contemporaries, shockingly radical. As Winnie Childs recalls:
'I remember the first brave unmarried father who said to Donald could he be present at the birth. So Donald was a bit shocked at first, then of course he was so delighted that he said ‘Certainly, yes certainly’. The talk that caused in the Queen Mother, that an unmarried father could be present at a birth'.
Nonetheless, for all his liberality, Donald was profoundly antipathetic to many aspects of modernity, especially where they challenged his idea of the correct relationship between the obstetrician and his patients.
It was not only the rising rates of abortion that Donald bemoaned. He was appalled at the prospect of artificial insemination by donor, which he regarded as morally the equivalent of adultery. In-vitro fertilisation, likewise, provoked him to fury:
'I have got involved in the raging debates coming out of in-vitro fertilisation. It is not as a treatment of a limited spectrum of female infertility that I deplore, nor any sense of pity I may have for the early human embryo subjected to experiment but to the sheer God-baiting arrogance of the so-called scientists and humanists that gets my goat that, to my mind, no sophistry can justify'.
He also disapproved of contraception for the unmarried:
'My hostility to the contraceptive pill is not based upon its alleged vascular effects nor even possible carcinogenic sequelae but on the sheer irresponsibility it introduces into sex.'
This is not to mention his opposition to divorce, to pornography, to euthanasia and to the use of cannabis.
In Donald’s view, in order fully to discharge his professional responsibilities the obstetrician had to be concerned not only with mother and fetus but with the moral, indeed the spiritual, welfare of society as a whole:
Will the gynaecologist of tomorrow, I wonder, be able to withstand the humanist pressure groups, that we may, in the words of a famous Anglican Collect, ‘So pass through things temporal that we lose not the things that are eternal.’ Or will we simply fall in with the new philosophy of expediency, to supply contraception without advice, abortion when contraception fails, and a neutral attitude towards the vagaries of human behaviour. Would this be failing the traditional role of guide, philosopher and friend to our patients?
Looking back with nostalgia to a golden age in which doctors occupied a more elevated moral position is, as Lawrence has pointed out, a common motif in the discourse of many medical holists, such as Lord Horder.
I hope I have not made too much of these similarities between Donald and Lord Horder. Certainly it is a comparison that could be pressed too far. But what the comparison with Lord Horder and his clinical and social holism does do is highlight some aspects of Donald’s life and work which might otherwise be missed or dismissed as not of great importance. To compose a full account of Donald we must, in other words, look beyond ultrasound. We must, as my title suggests, look beyond his work in the clinic. But in looking beyond the clinic we must not leave the clinician behind. I hope that I have done enough in this lecture to convince you that with Donald, as with Lord Horder, there is a real historical continuity between the diagnostician and the moralist. They are two sides of the same coin, two means to the same end. For better or for worse, they were two ways in which Donald sought to express what was a unified concern – a concern for his patients, body and soul, and for the society which they inhabited.
References
1. This essay is the revised text of the Goodall Memorial Lecture, given to the Royal College of Physicians and Surgeons of Glasgow, 5th June 2000. I am most grateful to Mr John Fleming, Honorary Collection Co-ordinator of the British Medical Ultrasound Society’s Historical Collection, for his assistance with the preparation both of the spoken lecture and this electronic version. I would also like to thank Dr Ian Spencer whose excellent work as research assistant greatly assisted the clarification of the aspects of Donald’s life and opinions here discussed.
2. Letter, I. Donald to Stasia [Anastasia Gardiner], 29 August 1978. All correspondence quoted from is in the BMUS Archive at The Queen Mother’s Hospital, Glasgow.
3. Ibid.
4. Donald published personal accounts of his second and third cardiac operations, I. Donald (1976) ‘At the receiving end: a doctor’s personal recollections of second-time cardiac valve replacement’, Scottish Medical Journal, 21, 49-57; Anon (1969) ‘At the receiving end: a doctor’s personal recollections of cardiac valve replacement’, Lancet, 2, 1129-1131.
5. Letter, I. Donald to F. Szontágh, 19 June 1974.
6. I. Donald (1978) ‘Report on the Nordic Obstetric Congress, Bergen, 1978’, unpublished typescript in BMUS Archives.
7. A. Munro, interviewed by Ian Spencer, 19 April 1997. Transferred to print, the meaning of the first sentence quoted may be obscure. Dame Alison meant that her brother and Dennis Hill were friends, while both were students at St. Thomas’s.
8. I. Donald, J. MacVicar, T. G. Brown (1958) ‘Investigation of abdominal masses by pulsed ultrasound’, The Lancet, 1, 1188-95.
9. See, for example, R. Reid (1977) My Children, My Children: Life before and after birth, an account of some recent developments, London, British Broadcasting Corp.
10. I. Donald, (1979) ‘An unstable subject’, B.M.J., 1, 604-5, p 604.
11. Letter, Donald to A. Sjövall, 24 January 1976.
12. This list is substantially taken from C. Lawrence (1998) ‘Still incommunicable: Clinical holists and medical knowledge in interwar Britain’, in C. Lawrence and G. Weisz (eds) Greater than the Parts: Holism in biomedicine, 1920-1950, Oxford University Press, London. See also C. Lawrence (1985) ‘Incommunicable knowledge : science, technology and the clinical art in Britain, 1850-1914’, Journal of contemporary history, 20 503-520 and idem (2000) ‘Edward Jenner’s Jockey Boots and the Great Tradition of English Medicine, 1918 to 1939’, in C. Lawrence and A.-K. Mayer (eds) Regenerating England: Science, medicine and culture in inter-war Britain, Amsterdam, Rodopi.
13. For biographical details of Lord Horder, see M. Horder (1966) The Little Genius: A memoir of the first Lord Horder, London, Duckworth.
14. W. Childs interviewed by Ian Spencer and John Fleming, July 1997; J. MacVicar, pers. com.
15. See also I. Donald (1977) ‘Superfecundity’, B.M.J. 1, 550-60.
16. Image from BMUS Historical Collection.
17. I. Donald (1961) ‘The New Yorkhill Maternity Hospital’, Scottish Medical Journal, 6, 164-69.
18. M.C.M[acnaughton]. (1987) ‘I Donald, CBE, FRCOG, FRCSGLAS, MD’, B.M.J. 2, 126.
19. Image from BMUS Historical Collection; the photograph was probably taken in 1979, when Donald was presented with an award by the charity, Action Research for the Crippled Child, in recognition of his services to obstetrics and neonatology.
20. Interview, Munro; W. Barr, interviewed by Ian Spencer and John Fleming, April 1996.
21. Image from BMUS Historical Collection.
22. I. Donald (1978) ‘Opatija speech’, unpublished transcript in BMUS archives.
23. This image was also used as the frontispiece of the fifth edition (1970) of Donald’s textbook, Practical Obstetric Problems, Lloyd-Luke, London. The caption was ‘Diasonograph ultrasonogram (Nuclear Enterprises Ltd) of normal fetus of twelve-and-a-half weeks gestation (menstrual age).
24. I. Donald (1969) ‘On launching a new diagnostic science’, American Journal of Obstetrics and Gynaecology, 103, 609-628.
25. From BMUS Historical Collection. An image very similar to the one reproduced here may be found in D.H. Howry, et al, (1955) ‘Ultrasonic visualization of living organs and tissues’, Geriatrics, 10, 123-28.
26. Ibid., pp 611-2.
27. Image in BMUS Archive, also published in I. Donald, J. MacVicar, T. G. Brown (1958) ‘Investigation of abdominal masses by pulsed ultrasound’, The Lancet, 1, 1188-95.
28. The most detailed account of this case is in J. MacVicar (1959) ‘Ultrasound as a diagnostic aid in obstetrics and gynaecology’, unpublished M.D thesis, University of Glasgow, p.127. See also I. Donald, J. MacVicar, T. G. Brown (1958) ‘Investigation of abdominal masses by pulsed ultrasound’, The Lancet, 1, 1188-95.
29. I. Donald (1969) ‘On launching a new diagnostic science’, American Journal of Obstetrics and Gynaecology, 103, 609-628, caption to fig. 16.
30. I. Donald (1974) ‘Apologia: how and why medical sonar developed’, Annals of the Royal College of Surgeons of England, 54, 132-140, p. 138.
31. I. Donald, (1979) ‘An unstable subject’, B.M.J., 1, 604-5.
32. Letter, I. Donald to J.H. Holmes, 14 June 1976.
33. I. Donald (1980) ‘Sonar: its present status in medicine’, in A. Kurjak (ed), Progress in Medical Ultrasound, Volume I, Amsterdam, Excerpta Medica.
34. Ibid.
35. I. Donald (undated but after 1978) ‘Predicting ovulation’, unpublished lecture, tape-recording in BMUS Archive.
36. Ibid.
37. Letter, I. Donald to Cecil (no surname given), 24 May 1979.
38. Letter, I. Donald to R. Algranati, 3 May 1979.
39. On occasion, Donald would show the woman seeking a termination his film of fetal movement; on other occasions, he would organise an ultrasound scan of her fetus.
40. Interview, Childs.
41. Letter, I. Donald to Peggy (no surname given), 15 August 1980.
42. I. Donald (1977) ‘Does Christianity Help’, pamphlet published by the Order of Christian Unity, London, copy in BMUS Archives; see also Letter, I. Donald to J.J. Scarisbrick, 23 March 1976. He differed in this respect from the standard Catholic absolutist position of opposition to all abortions.
43. Microcephaly is a good example of the type of condition for which Donald was prepared to offer the mother a termination.
44. S. Campbell, pers. com; Interview, Barr.
45. I. Donald (1972) ‘Naught for your comfort’, Journal of the Irish Medical Association, 65, 279-89.
46. I. Donald (1977) ‘Does Christianity Help’, pamphlet published by the Order of Christian Unity, London, copy in BMUS Archives; see also I. Donald (1979) ‘Speech on accepting the Harding Award’, typescript in BMUS Archive.
47. Letter, I. Donald to R. Fliequer, 13 January 1978.
48. I. Donald (1972) ‘Naught for your comfort’, Journal of the Irish Medical Association, 65, 279-89.
49. Interview, Childs.
50. I. Donald (1985) ‘Problems raised by artificial human reproduction’, unpublished talk given at Robertson House, Edinburgh, 19 January 1985, typescript in BMUS archive.
51. Letter, I. Donald to T. Chow, 1 August 1985.
52. Ibid.
53. B. Nash (1978) ‘Daughters in danger: Professor Ian Donald talks to Barbara Nash’, Mother, April, 343-36. See also I. Donald (1974) ‘Life, Death and Modern Medicine’, pamphlet published by the Order of Christian Unity, London, copy in BMUS Archives; Letter, I. Donald to T. Donald, 5 March 1970; and the following reference.
54. I. Donald (1972) ‘Naught for your comfort’, Journal of the Irish Medical Association, 65, 279-89.

Support us
As a charity we rely on your donations to fund our free exhibitions, school activities and online resources